Overtreatment in IVF: A Senior Fertility Specialist’s Perspective
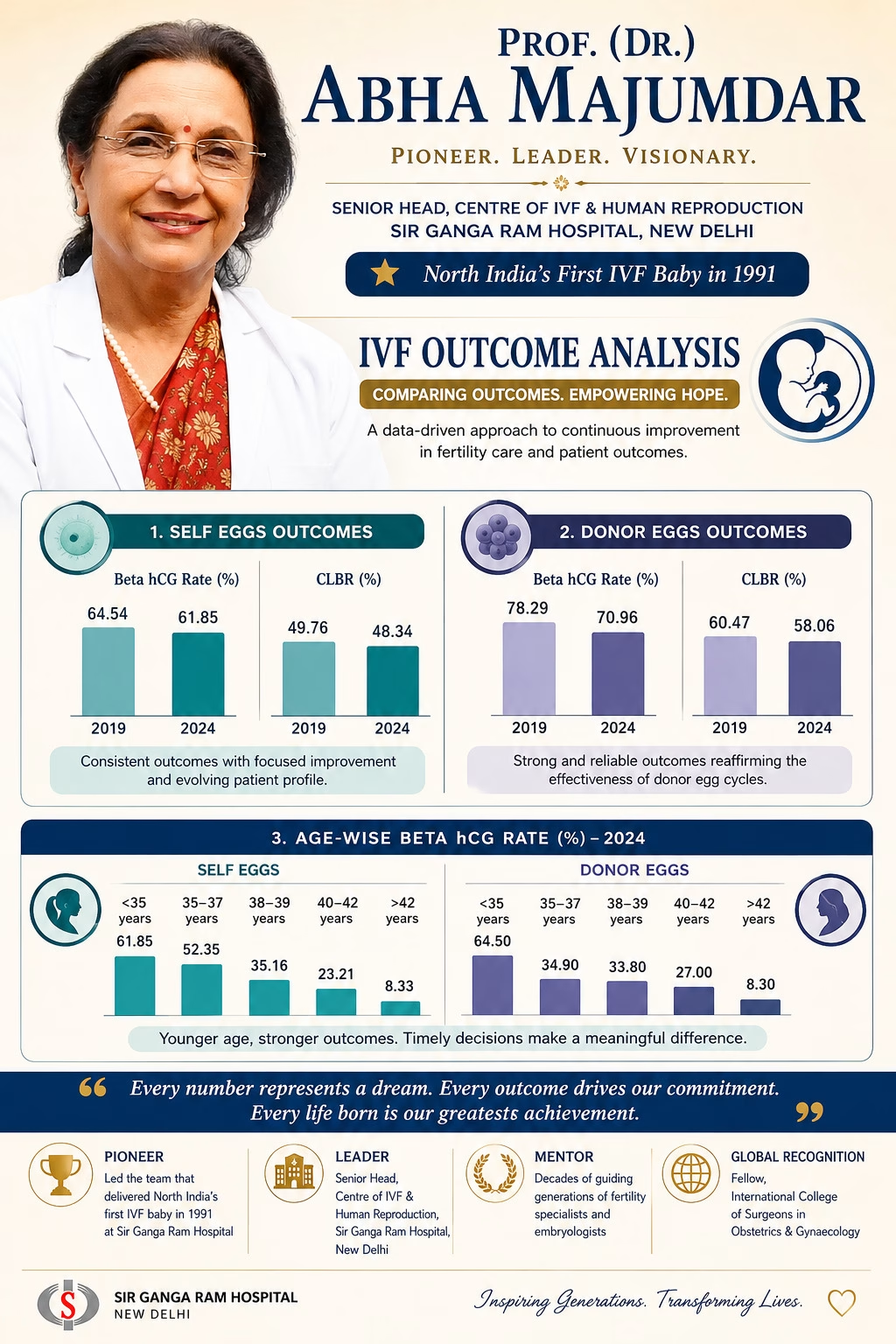
Having spent more than 40 years in reproductive medicine—and having had the privilege of helping deliver North India’s first IVF baby at Sir Ganga Ram Hospital in 1991—I have seen firsthand the incredible evolution of fertility treatments. While science and technology have advanced rapidly, one core principle must remain unchanged: Do what is necessary, not what is excessive.
This conviction is why we need an honest conversation about a growing concern in modern fertility care: overtreatment in IVF, specifically the routine use of unproven “treatment add-ons.”
When “More” is Mistaken for “Better”
In vitro fertilization (IVF) and intrauterine insemination (IUI) are established, core treatments that have been proven effective for most patients. However, overtreatment happens when we mistake more intervention for better care. It can take many forms:
- Starting IVF too early, even when natural conception remains possible.
- Ordering excessive investigations that create anxiety but do not change clinical outcomes.
- Prescribing multiple medications without proven additional benefits.
- Routinely recommending optional, non-essential “add-ons” under the assumption that they act as “implantation boosters.”
The very term ‘add-on’ suggests ‘extra benefit’. But medicine must be guided by evidence—not assumption. Leading regulators, such as the ‘Human Fertilization and Embryology Authority’ (HFEA for UK) have repeatedly highlighted that for most patients, routine cycles of proven fertility treatment are highly effective ‘without’ using any treatment add-ons.
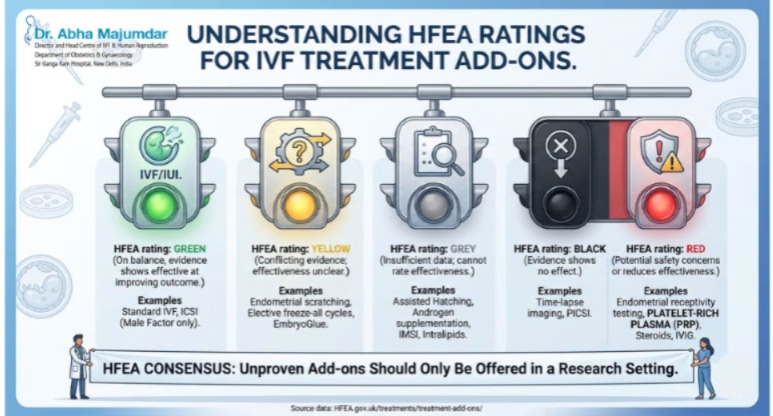
Understanding the Evidence: The HFEA Traffic-Light Ratings
To protect patients and bring transparency to the field, the HFEA’s Scientific and Clinical Advances Advisory Committee (SCAAC) reviews published data and categorizes common add-ons using a strict traffic-light rating system.
When clinics routinely suggest these procedures, patients must understand where they stand on the scientific spectrum:
When is it Appropriate to Use a Treatment Add-on?
This evidence should make all of us pause, but it does not mean add-ons have no place in medicine. There are valid nuances to consider:
- Justifiable Medical Redirection: An add-on may be offered for reasons other than simply increasing the live birth rate. For example, specific protocols might be justified if they significantly reduce the risk of a miscarriage such as with natural ovulatory cycle for frozen embryo transfer or mitigate the threat of Ovarian Hyperstimulation Syndrome (OHSS) in a specific high-risk patient by using antagonist protocol with agonist trigger and freeze all policy.
- Strictly Monitored Subgroups: Certain procedures are authorized only for highly selected cohorts. For instance, ‘Artificial oocyte Activation by using Calcium Ionophore carries potential chromosomal risks and is not meant for routine use, but it may be justified for patients with specific cellular deficiencies (like PLC zeta deficiency) or those with severe, repeated fertilization failure.
- Research, Not Retail: Treatments that lack strong evidence of safety or effectiveness ‘should only be offered within formal research setting or clinical trial’. Crucially, patients should never be charged extra to participate in research.
If you are paying out-of-pocket, it is frequently more effective to save those financial resources to fund a subsequent, clean routine IVF cycle rather than exhausting your savings on unproven add-ons for a single cycle.
The Rise of “Package-Driven” IVF
Compounding the issue of clinical overtreatment is the commercialization of fertility care. Today, vulnerable patients are frequently influenced by retail-style marketing: discounts, festival offers, “guaranteed packages,” and free gifts.
But IVF is a medical journey, not a retail transaction. A “cheaper package” headline often masks hidden lines. It may completely exclude:
- Essential medications and stimulation hormones
- Embryo freezing and long-term storage charges
- Anesthesia and operating theatre fees
- Advanced laboratory procedures or repeat ultrasound monitoring
These financial layers often appear later—at a point when patients are already emotionally and physically invested. Patients deserve absolute, unambiguous financial transparency from day one.
Empowering Couples: Questions to Ask Your Clinic
Before committing to a fertility clinic, look past the marketing and ask the hard, clinical questions:
- What is your live birth rate, not just your chemical pregnancy rate?
- What is your age-specific outcomes for someone like me?
- Is this protocol being explicitly individualized for my unique condition, or is it a standard clinic protocol?
- Why am I being recommended this specific add-on, and what specific evidence supports its use for my case?
- What is the quality and accreditation of your embryology laboratory?
A good clinic explains; it does not pressurize. A good doctor informs; they do not frighten.
My Philosophy After Decades in IVF
Technology is valuable and innovation is welcome. But wisdom in reproductive medicine lies in knowing when not to intervene unnecessarily. My favorite quote as an ob./gyn and reproductive clinician which I have pragmatically followed all my life is ‘Masterly inactivity and timely intervention’.
Good IVF is not about doing the most; it is about doing what is right—for the right patient, at the right time, and for the right clinical reason. Patients are not purchasing a commercial product. They are placing their vulnerability, their trust, and their deepest dreams of parenthood into our hands. That trust must always be honored with rigorous science, uncompromised ethics, and genuine compassion.
